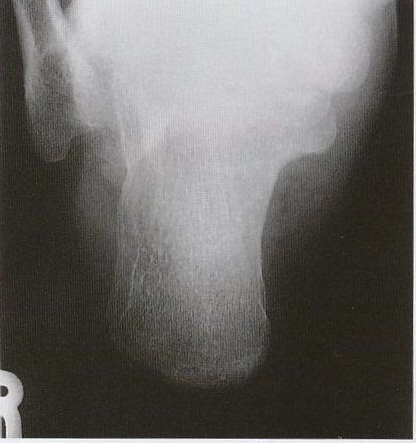
CALCANEUS AXIAL PROJECTION
Axial View • Complete Calcaneus Evaluation • Posterior Tuberosity to Talocalcaneal Joint

Exposure Factors
Equipment: Without bucky. Position: Supine or seated.
Note: Higher kV for adequate penetration of dense calcaneus bone
Plate Size
DORSIFLEXION OF FOOT
Dorsiflex foot so plantar surface is almost perpendicular to cassette.
This position is critical for adequate calcaneus visualization
GAUZE TRACTION
Place gauze band under foot and ask patient to:
- Apply gentle but firm traction
- Keep plantar surface as perpendicular to cassette as possible
- Maintain position throughout exposure
CENTERING POINT
Directed to base of third metatarsal to exit distal to lateral malleolus
Calcaneus Anatomical Structures
Posterior Tuberosity
Posterior part of calcaneus, Achilles tendon insertion
Calcaneus Body
Main bone body, denser
Talocalcaneal Joint
Articulation with talus (posterior ankle)
- Calcaneal tuberosity - Posterior part, Achilles tendon insertion
- Calcaneus body - Main bone mass
- Sustentaculum tali - Medial projection supporting talus
- Calcaneal sulcus - Inferior groove
- Posterior talocalcaneal joint - Posterior articular surface with talus
- Anterior and middle talocalcaneal joints - Anterior articular surfaces
- Lateral tubercle - Lateral projection
- Medial tubercle - Medial projection
- Superior and inferior borders - Bone contours
- Bone density - Evaluation of largest foot bone density
Patient Positioning
40° CEPHALIC ANGLE
40° cephalic direction to longitudinal foot axis
Central Ray Direction
40° cephalic directed to base of third metatarsal
Entry point: Base of third metatarsal
Exit point: Level immediately distal to lateral malleolus
Angulation: 40° cephalic direction to longitudinal foot axis
Objective: Complete calcaneus visualization from posterior tuberosity to talocalcaneal joint
IMPORTANT: FOOT POSITION
The foot dorsiflexion to achieve plantar surface perpendicularity is essential for:
- Adequate visualization of entire calcaneus
- Avoiding overlap with other structures
- Correct bone orientation for axial projection
- Optimization of 40° central ray angle
Without this position, projection will be inadequate
Patient Instructions
"Remain still during examination"
"Maintain gentle but firm traction with gauze"
"Keep foot in flexed position"
Technical Considerations
40° Angle
40° cephalic angulation essential for axial calcaneus visualization.
Dorsiflexion
Foot dorsiflexed with plantar surface perpendicular to cassette.
Gauze Traction
Gauze use to maintain position and facilitate traction.
Elevated kV
70 kV necessary to penetrate dense calcaneus bone.
Clinical Indications
Image Quality Criteria
Complete Calcaneus
Entire calcaneus visible from tuberosity to talocalcaneal joint
No Rotation
Calcaneus centered without lateral or medial rotation
Adequate Density
Adequate penetration of dense calcaneus bone
Correct Angle
40° cephalic angulation correctly applied
Calcaneus and Ankle Study
COMPLEMENTARY PROJECTIONS
For complete ankle and posterior foot evaluation:
Calcaneus axial projection is essential for fracture and heel pathology evaluation
Special Technical Note
ELEVATED KILOVOLTAGE (70 kV)
Calcaneus requires higher kV (70 kV) due to:
- High bone density - Largest and densest foot bone
- Significant thickness - Requires greater penetration
- Complex trabecular structure - Needs adequate contrast
- Low mAs (5) - Compensates with higher kV to maintain exposure
- Fine detail visualization - Articular structures and trabeculae
In osteoporotic or less dense bone patients, consider slightly reducing kV